
Older people who are struggling with obesity soon will be able to get highly effective weight loss drugs for $50 a month, far less than popular drugs like Zepbound and Wegovy currently cost.
These drugs are what’s known as GLP-1s, just like Ozempic, the popular diabetes medication that kicked off a revolution in the pharmaceutical industry and inspired as many as 12% of people in the U.S. to try using weight loss drugs. (GLP-1 stands for glucagon-like peptide-1, a natural hormone that people produce in their guts. It helps slow digestion and reduce food cravings.)
Millions of people in the U.S. could be eligible to participate in the new Medicare pilot program, which is scheduled to begin on July 1 and is called the Bridge program.
Altogether, 70.1 million Americans currently are enrolled in Medicare, the federal government health insurance program for adults ages 65 and older. And in the U.S., nearly 70% of adults are either overweight or obese. Not every overweight Medicare recipient will qualify for the new, cheaper weight loss drugs, so it will be important for patients and their doctors to pay attention to all the details.
But the impacts of this new drug coverage likely will be dramatic as millions of Americans flock to their primary care providers to seek new GLP-1 prescriptions or to switch to the Bridge program to save hundreds of dollars a month on weight loss drugs.
“This is a big step forward in prevention of health challenges for our Medicare population. These drugs have incredible potential benefits,” said Dr. Annie Moore, an internal medicine doctor who is board-certified in obesity medicine and has extensive experience prescribing GLP-1 weight loss medications to her patients.
“This pilot will be a huge social and healthcare experiment. Never before have we rolled out drugs like this to so many people,” Moore said.
We talked with Moore to learn more about how the new Bridge program will work and to answer your top questions.
Who qualifies for Medicare GLP-1 weight loss drugs for $50 a month?
To qualify for the Medicare GLP-1 Bridge program, patients must be classified as “obese,” meaning they have a body mass index (BMI) of 30 or greater.

“The program is covering medications only for people who meet the definition of obesity, not for those who are overweight,” Moore said. “I’m supportive of that because carrying a little extra weight when you’re 65 or older is not a bad thing. And the health risks related to obesity really start to increase with BMIs of 30 or greater.”
Moore cares for patients at CU Internal Medicine – Cherry Creek in Denver and also is a professor at the University of Colorado Anschutz School of Medicine. She researches best practices in patient care through the Brown Moore Endowed Chair for Excellence in Patient Experience.
Moore studied obesity medicine before the recent GLP-1 revolution in weight loss drugs, has practiced medicine for nearly 40 years and has been prescribing GLP-1 drugs to many of her patients over the past 5 years.
Obesity has been a growing epidemic in the U.S. for decades.
About 40% of adults in the U.S. are obese, with BMIs of 30 and higher. Among those people, about 10% are severely obese, meaning they have BMIs of 40 or greater. An additional 25% of U.S. adults are overweight, with BMIs of 25 to 29, according to data from the U.S. Centers for Disease Control and Prevention (CDC). The percentage of obese adults climbs to 68% if medical experts consider waist size along with BMI.
Eligibility details for Medicare GLP-1 weight loss drugs under the new Bridge program:
- People with BMIs of 35 or greater.
- People with BMIs between 30 and 35 who also have additional health problems, including:
- Heart failure.
- Uncontrolled high blood pressure or hypertension.
- Chronic kidney disease.
- People with BMIs of 27 or higher who previously have had:
- Heart attacks.
- Strokes.
- Pre-diabetes.
- Peripheral artery disease, which causes narrowing of arteries.
People ages 65 and older who are overweight — meaning they have BMIs between 27and 30 — generally will not qualify for the lower-cost GLP-1 drugs through the Bridge program.
Do you need a Medicare Part D plan to get GLP-1 weight loss drugs at a discounted price?
Yes. In order to get the GLP-1 weight loss drugs for $50 a month, patients will need to have optional Medicare Part D drug plans. People purchase these plans through private insurance companies as supplements to their regular Medicare coverage. (Learn more about Part D.) Typically, the private insurance companies that sell Part D plans to Medicare recipients cover the costs of medications for Part D recipients, but the Bridge program is unique. Because federal officials anticipate that millions of people may want to try GLP-1 medications under the pilot program, and they expect the program to be very expensive at first, federal funding will cover the cost of the Bridge program for the first 18 months, including the second half of 2026 and all of 2027.
“Usually, you have an insurance provider. But CMS (the Centers for Medicare and Medicaid Services) is taking the risk financially for the first 18 months, not the insurer,” Moore said. “That’s why they’re calling it the Bridge program.”
Which GLP-1 weight loss drugs will Medicare cover?
Doctors will have to prescribe specific versions of the weight loss drugs to help patients qualify for the $ 50-per-month price.
GLP-1 medications included under the Medicare Bridge program:
- Zepbound – a once-weekly needle injection.
- Wegovy – both once-weekly needle injections and daily pills.
- Foundayo, a new once-daily pill from the makers of Zepbound.
The most well-known weight loss drug in recent years has been Ozempic, but it’s not actually a weight loss drug. Danish pharmaceutical company Novo Nordisk started making Ozempic to help people with diabetes. But the drug became a blockbuster when patients and doctors discovered that, in addition to helping with diabetes, the drug also causes people to lose a significant amount of weight.
The generic name for the drug is semaglutide, and Novo Nordisk started making new forms of the drugs that are specifically for people who want to lose weight. This version is called Wegovy, and it now comes in an injection that people take once a week or a daily pill.
The newer popular drug for those wanting to lose weight is called Zepbound. American drug manufacturer Eli Lilly started making drugs to compete with Ozempic and Wegovy. The generic name for the drug in Zepbound is tirzepatide. It helps people lose an even higher percentage of weight than people typically lose when they take Ozempic and Wegovy, so Zepbound has surged in popularity over the last couple of years. When people take tirzepatide for diabetes, the drug is called Mounjaro.
The Medicare GLP-1 Bridge program will cover Zepbound, but only when doctors prescribe a version called the KwikPen. It’s an injector pen that patients use to give themselves once-weekly shots. Each KwikPen contains four doses, so one pen works for one month. In the past, people who took Zepbound used single-injection pens and needed four of them each month. Others received vials with liquid tirzepatide and used needles and syringes to load and inject Zepbound.
Under the Medicare program, patients also will be able to take Foundayo, the new pill that Eli Lilly is manufacturing. Foundayo is made with a different drug called orforgilpron.
The drug makers expect pill forms of GLP-1 medications to be popular with patients because some are afraid of needles and don’t like injecting themselves with medications. But Moore said very few of her patients are using the pills. That’s because it can take a long time to build up to a high enough dose where patients lose weight. The pills seem to cause similar side effects to injections without causing as much weight loss, Moore said.
The newest weight-loss drug, called retatrutide, could help people lose 30% of body weight, based on recent clinical trials. Federal regulators have not yet approved the medication.
What are the pros and cons of GLP-1 weight loss drugs?
The biggest benefit of GLP-1 weight loss medications is that they help people lose significant weight. The medications also have been proven to reduce the risk of strokes and heart attacks for people with cardiovascular problems. And they can eliminate sleep apnea, can help curb cravings for alcohol and drugs and show great promise in reducing cancer risks.
On the flip side, the drugs can cause gastrointestinal problems including diarrhea, constipation, nausea and vomiting. Medical providers can help people start with the least potent doses and gradually work up to stronger versions of the medications. This is known as “titrating” doses. Many patients tell Moore that they get used to the side effects. But others stop taking the drugs. Studies have shown that at least 50% of people who take GLP-1 medications stop using them within one year. Researchers don’t know why people stop using the drugs. They suspect that both cost and negative side effects cause people to stop using the drugs.
Bone health is also a concern, especially for women in menopause who are already at risk for bone loss. Weight loss can cause bone loss for anyone.
If cost is a central factor, the Medicare program may have a big impact.
Until now, GLP-1 drugs have been extremely expensive, and most insurance companies have not covered the drugs. They initially cost between $1,200 and $1,500 a month. The costs then declined to about $450 to $500 per month. The Bridge program could further reduce costs for all patients, including those not on Medicare.
That’s because private insurance companies often follow suit after Medicare starts covering medications, Moore said.
Do people with diabetes qualify for the Medicare GLP-1 weight loss drugs?
No. The Bridge program applies only to people with obesity. Medicare recipients with diabetes already have coverage for drugs like Ozempic and Mounjaro, so they won’t be eligible for the new GLP-1 Bridge program.
If you’ve lost weight with GLP-1s, can you still qualify for the new program?
Yes. The Bridge program rules say that people can use the drugs to “maintain weight loss.” That’s because doctors have found that if people successfully lose weight using GLP-1 medications, then stop taking the drugs, they typically gain the weight back. In order to keep weight off, people need to continue taking the GLP-1 medications indefinitely.
“Patients need to stay on these drugs,” Moore said. “We’re still not sure what the maintenance models will look like: possibly less frequent dosing. But that’s being evaluated in a lot of research right now.”
Will older people in Colorado qualify for Medicare GLP-1 weight loss drugs?
Colorado has the lowest percentage of people in the U.S. who are overweight and obese, according to data from the U.S. Centers for Disease Control and Prevention (CDC). But even in Colorado, where people love to spend time outdoors and stay active, the percentage of people who are struggling with obesity has continued to rise for decades.
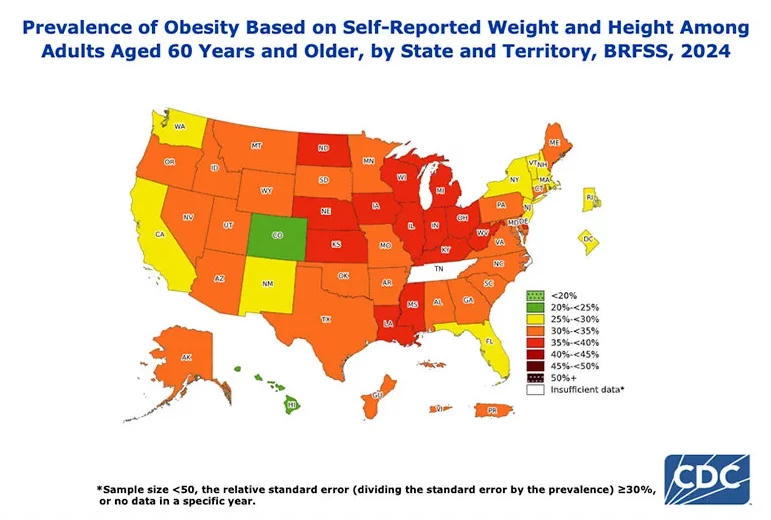
Where are the obesity rates highest in the U.S.?
- The highest obesity rates are in the Midwest and the South. In the Midwest, nearly 36% of people are obese, while nearly 35% of people in the South are obese.
- About 30% of people in the West and in the Northeast are obese.
- As of 2024, Colorado had an obesity rate of 25%. That number has been climbing for decades. Back in 1990, fewer than 10% of Coloradans were obese.
- The states with the highest obesity rates are Mississippi and West Virginia, where more than 40% of people are considered obese.
- People of color have higher obesity rates in the U.S. compared to others. On average, 33% of Hispanic adults are obese, while 41% of Black adults are considered obese. Asian adults have the lowest obesity rates in the U.S.
Why is Medicare expanding access to GLP-1 weight loss drugs?
The short answer is that GLP-1 drugs have been very popular because they work well and help people lose as much as 21% of their body weight. But they’ve also been extremely expensive.
Furthermore, the 2003 law that created Medicare Part D barred coverage of weight loss drugs. Since the newest drugs have proven so effective — both at helping people lose weight and preventing other health problems — doctors and policymakers want to expand access to GLP-1 medications.
“This pilot program is a reversal of the 2003 law (which barred Medicare coverage for weight loss drugs), and we need to applaud that,” Moore said.
Still, the new Bridge program will be an experiment. And the launch could be challenging, since so many people may try to get GLP-1 prescriptions all at once soon after the July 1 launch.
Moore said she is concerned there may be logistical challenges and that Medicare recipients should brace for possible frustrations and delays. She’s urging patients to be patient if they’re trying to get new prescriptions under the Bridge program.
What should Medicare recipients do if they think they qualify for GLP-1 weight loss drugs?
Patients interested in trying GLP-1 weight loss drugs will need to visit their primary care providers to determine eligibility. There could be some delays because patients will need to undergo a verification process known as “prior authorization” to determine whether they qualify for the low-cost drugs.
Will doctors be able to handle increased demand for GLP-1 weight loss drugs?
Yes. Moore said primary care providers who aren’t familiar with prescribing GLP-1 medications may struggle at first.
Patients need a lot of information and support when they’re taking the drugs. They need to gradually get used to higher and higher doses. And they need to learn how to inject the medications (or need to commit to taking a daily pill).
Moore said providers who are part of larger systems, like she is, will have more support. UCHealth pharmacy experts handle prior authorization requests for all University of Colorado clinics.
“I wonder about primary care providers with small offices. Will they have the staff to deal with the initial surge?” Moore said. “I think this will be particularly challenging over the first six months of the program.”
Will low-income people have better access GLP-1 weight loss medications?
Yes. Moore hopes that the Bridge program will give lower-income people and people of color much better access to GLP-1 medications than in the past.
“These drugs have been unaffordable for many people,” she said.
If cost were not a barrier and patients could connect with primary care providers who could help them obtain necessary authorizations, many more would be able to take advantage of the Bridge program.
Moore does worry, however, that $50 per month co-pays, while much less expensive than previous prices for the drugs, may still be out of reach for some of the neediest Americans.
“This is huge step forward for equity, but I still wonder what percentage of our Medicare population can afford $50 a month,” she said.
Some patients may need to wait for generic GLP-1 medications, which eventually will arrive on the scene.
If GLP-1 drugs are so expensive, why is Medicare expanding access?
People who are losing a significant amount of weight with GLP-1 drugs have fewer health problems. And as competition for these drugs increases, the cost of these drugs continues to go down.
Moore said health policy experts are hoping that if more people who are struggling with obesity can afford GLP-1 medications, they might lose significant amounts of weight, and their health might improve dramatically.
The goal is to spark dramatic change over the long run.
“They’re hoping to see cost savings,” Moore said. “With weight loss, we’ll likely see health improvement and a reduction in complications that diabetes and other health problems cause.”
The launch of the Bridge program marks a major paradigm shift.
“Medicare has historically been about ‘sick care’ rather than ‘healthcare,’” Moore said. We have not covered preventive care as well. Assuming this pilot is successful, which I hope it is, we may later look at this moment as an inflection point when we moved from a reactive, sick-care model to a prevention-based model.”
Why have obesity rates risen so dramatically in the U.S.?
Highly processed foods have become much more common in recent decades, and Moore and others think they’re the chief drivers of the obesity epidemic. When people are hungry, it’s easiest to reach for processed foods rather than taking the time to cook healthy meals with plenty of fresh fruits, vegetables, legumes, nuts and healthy proteins.
Sedentary lifestyles also are to blame, Moore said.
But the success of GLP-1 medications has underscored that brain chemistry plays a big role for people who are obese or overweight. People who gain weight easily are responding to signals within their brains. They’re eating because they’re hungry.
GLP-1 drugs are so effective because they reduce hunger and cravings. Patients can fill up on smaller amounts of food.
What are you seeing among patients using GLP-1 weight loss medications?
Moore said she sees patients nearly every day who have lost up to 70 pounds each on GLP-1 medications.
Most are healthier and more active.
“If you’re not carrying an extra 70 pounds, it’s so much easier to move,” she said. “Most people love the fact that they’re not having to suppress food noise and constantly fighting the urge to not eat things that aren’t healthy.
“Overall, if they can afford the medication, they are overwhelmingly thrilled,” she said. “It doesn’t mean that they don’t have a few side effects, but they say that the trade-off is very worthwhile.”
Moore expects newer generations of GLP-1 medications to continue improving.
While Ozempic may always be the generic term for these drugs, just like we ask for Kleenex when we want a tissue, Moore expects that medical providers and researchers will look back 10 or 15 years from new and see Ozempic as a “pretty dated drug.”
There is even talk about people someday getting little implants in their bellies that will gradually release GLP-1s to help control appetite without the need for pills or injections.
“This will be a huge field,” Moore. “There will be ripple effects in multiple industries like clothing and seating and alcohol. And I’m excited to watch it all.”